The Nurse Reviews the Pathophysiology of Scoliosis With the Student Nurses
Continuing Education Activity
Boyish idiopathic scoliosis (AIS) is the near mutual form of pediatric scoliosis occurring in individuals betwixt the ages of 10 to 18. By definition, idiopathic scoliosis implies that the etiology is unknown or not related to a specific syndromic, congenital, or neuromuscular condition. Treatment options include conservative management, bracing, or operative intervention. This action outlines the evaluation and direction of adolescent and idiopathic scoliosis and highlights the office of the interprofessional team in treating patients with this status.
Objectives:
- Review the imaging evaluation of adolescent and idiopathic scoliosis.
- Summarize the treatment of boyish and idiopathic scoliosis.
- Outline the postoperative rehabilitation for patient with adolescent and idiopathic scoliosis.
- Summarize the importance of collaboration and communication among interprofessional team members to enhance care coordination for patients with adolescent and idiopathic scoliosis.
Introduction
Adolescent idiopathic scoliosis (AIS) is the most mutual class of pediatric scoliosis. Information technology occurs in individuals between the ages of ten to eighteen. By definition, idiopathic scoliosis implies that the etiology is unknown or not related to a specific syndromic, congenital, or neuromuscular condition. Treatment options include conservative management, bracing, or operative intervention.[ane][2][iii]
Etiology
Idiopathic scoliosis is a diagnosis of exclusion of other forms of scoliosis. As of today, in that location is no identifiable cause for idiopathic scoliosis. Theories include hormonal causes, disproportionate growth, muscle imbalance, and genetic factors. Nearly xxx% of patients with AIS accept a family member with scoliosis.
Epidemiology
The prevalence is about 1% to 3% for AIS. There is a preference for females and a right-sided curvature. To exist considered for the classification of scoliosis the curve must be at least x degrees in the coronal plane. The prevalence is approximately 0.1% for curves measuring more than 40 degrees (those which tend to be those requiring operative intervention).
History and Physical
A thorough history and physical is warranted. Particular attention should be paid to the developmental history to dominion out any other etiologies of scoliosis. Attending must likewise be placed on questions focused on skeletal maturity including the age of menarche and determination of Risser classification. In a gross generalization, near adolescent patients presenting with idiopathic scoliosis will non have dramatic dorsum pain from the curvature. Many tend to be very active including athletes, cheerleaders, and otherwise very healthy children.[four][v][6]
The physical test must include a neurologic assessment as well every bit evaluation of the bend's shape, class, and flexibility. Patient privacy and sensitivity in this age demographic are of import to consider while ensuring proper evaluation of the spinal bend. Photographic documentation with the patient standing upright likewise as bending over is vital to runway progression every bit well as the operative outcome. Spinal curvature is not isolated to a spinal deformity. Rib prominence, waistline, and shoulder height should also be documented.
Evaluation
Evaluation is generally a screening evaluation either through a school entity, sports coach, or pediatrician. The proper formal evaluation includes x-ray imaging. Patients need a continuing coronal 10-ray, sagittal ten-ray, left and correct bending 10-rays. Risser nomenclature can more often than not exist calculated from the iliac crest on the coronal x-ray platform. Consensus holds that a CT scan and MRI imaging for typical AIS patients is not warranted. However, certain intraoperative imaging guidance techniques do crave either preoperative or intraoperative CT imaging. This is a surgeon and engineering specific. Patients who are pre-operative candidates undergo a standard laboratory workup including CBC, BMP, INR/PTT, urinalysis, and a urine pregnancy exam for all females.
Other tests should include pulmonary function tests.
Treatment / Management
Historically speaking, those with curves less than 10 degrees do non meet the specification for diagnosis of AIS. Furthermore, the United states of america Preventative Services Task Force has recently questioned whether school screenings positively touch the patient-centered-health outcomes.[7][8][9]
Generally speaking, those with curves of 10 to 25 degrees are monitored for surveillance with serial 10-rays. This is usually at 3, 6 or 12-month intervals.
Those with curves greater than 25 degrees only less than xl to 45 degrees are candidates for bracing. The Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) was an NIH funded randomized control trial that illustrated the effectiveness of bracing in the adolescent population. Even though braces are widely prescribed, these uncomfortable devices have low compliance rates and their overall success remains questionable. Questions take been raised virtually every blazon of brace for managing scoliosis.
Those with curves over 40 to 45 degrees who are skeletally young are operative candidates. The mainstay of operative treatment is surgical fusion. Historically this could be anterior or posterior fusion or a combined inductive-posterior approach. Currently, the leading technique is posterior fusion with pedicle screws and bilateral rod placement. Selection of operative levels is a circuitous determination algorithm taking into account coronal deformity location, regional kyphosis, shoulder meridian, L4 tilt, and lumbar alignment. Furthermore, a ratio comparing between the chief thoracic curve Cobb bending and the thoracolumbar bend Cobb angle also as the apical vertical translation and apical vertebral rotation must be considered for advanced operative planning.
New non-fusion techniques such as tethering procedures are gaining traction as well. Surgery for scoliosis is a major procedure and the literature is replete with serious complications that are even more disabling than the disorder itself.
Other treatments similar physical therapy, electrical stimulation, diet, and spinal manipulation have not been establish to be constructive in managing scoliosis.
These are gross generalizations, and actual patient intendance operative decisions must business relationship for patient-specific factors, skeletal maturity, deformity progression, patient'south socioeconomic factors, and surgeon experience.
Differential Diagnosis
It is essential to rule out scoliosis from other causes such as neurologic conditions, neuromuscular conditions, congenital, or syndromic issues.
Staging
The Lenke Nomenclature scheme best categorizes staging. The purpose of this classification scheme is to create a uniform approach to naming and described curves. The overall intent at an advanced level is also to give some preference for the operative handling protocol.
The Lenke Classification takes into account the coronal curve (1-vi), the sagittal deformity (-, N, or +), and the lumbar spine modifier (A, B, C). This creates a descriptor such as 3C+ or 1B-. Formal education of the Lenke classification and memorization of the criteria is beyond the scope of this text. However, information technology is the preferred method for spinal deformity surgeons to communicate about AIS.
Prognosis
Patients with adolescent idiopathic scoliosis that become untreated into adulthood tin take a rate of progression that is approximately 0.5 to 1 degree per year once the patient has reached a 50-caste coronal angle. Furthermore, in gross generalization, curves in adulthood tend to be much stiffer and more rigid than in the adolescent cohort requiring more than aggressive and invasive surgical techniques.
Long term studies report a higher rate of arthritis and poor perception of trunk image in patients with scoliosis, irrespective of treatment. Further, if the surgical correction involves chest wall invasion, it may also consequence in hurting and decreased lung function.
Complications
Complications from untreated scoliosis include deformity progression. This can generate back hurting, lumbar radiculopathy, cosmetic problems, nerve damage, and even cardiac and pulmonary restriction. Untreated patients with a bend of more than 80 degrees in the coronal plane can have increased shortness of breath.
Surgical complications are generally lower than in adult spinal deformity surgery but present. Ane national information series estimated the post-surgical neurologic injury at 0.9%, respiratory complications at 2.viii%, cardiac complications at 0.8%, infection at 0.five%, and 2.seven% for gastrointestinal complications. Delayed infections in the hardware are as well common.
Surgeon expertise and volume of surgery are also of import factors regarding the outcome and cost of surgery.
Postoperative and Rehabilitation Care
Patients are managed in an ICU post-obit surgery and depending on the extent of surgery, some crave a prolonged stay.
Most patients undergoing adolescent idiopathic scoliosis surgery are expected to return to home post-obit their operative intervention. Length of stay can vary based on the surgical procedure, surgeon preference, institutional algorithms, and other medical or socioeconomic sequel. Bracing is more often than not not needed every bit a mail-operative therapy.
Deterrence and Patient Education
Challenges exercise present in the management of bracing with this population. Furthermore, a written report has illustrated improved outcomes with increased compliance to bracing protocols. Adherence requires significant interest from both the patient and the patient'southward support structure. Furthermore, meaning education of the parents is required regarding operative adventure, operative planning, and purpose of the operative intervention.
Pearls and Other Issues
- The Lenke Classification creates the language used past experts to converse about scoliosis blazon. Information technology is the most common and widely used nomenclature scheme.
- To properly classify boyish idiopathic scoliosis proper imaging is essential.
- Pregnant enquiry is ongoing regarding the genetic factors related to curve formation and progression.
- Management of this disease etiology requires patient also every bit parent education to maximize outcome and create reasonable expectations.
Enhancing Healthcare Team Outcomes
The management of scoliosis is complex and the overall results are poor. Because the status results in a cosmetic and functional deformity it is best managed past an interprofessional team that includes a physical therapist, orthopedic surgeon, pulmonologist, rheumatologist and a neurologist. The vast majority of patients do non require surgery and can be managed with not-surgical therapies.
While braces are heavily prescribed, they take depression compliance because of the extreme discomfort. For those with functional deficits, physical therapy is recommended - this therapy has no impact on scoliosis - information technology just improves musculus and joint function. Afterwards surgery, nurses should encourage and educate patients regarding incentive spirometry to prevent atelectasis.
Surgery is recommended for symptomatic patients with severe deformity-just the patient needs to be educated nearly the complications of scoliosis which are not footling. After surgery, nurses should encourage incentive spirometry to prevent atelectasis. Surgery can ameliorate function and aesthetics but a meaning number of patients do remain with residuum pain or other neurological deficit that can reduce the quality of life.[vii][10][11]
A mental health nurse should consult with all patients because scoliosis tin can impart serious cosmetic deficits which lead to anxiety, withdrawal, and depression. Most patients with scoliosis do non accept part in sports for fright of embarrassment or humiliation.
Some degree of pain is present in patients with scoliosis but the fundamental is not to empirically prescribe prescription-force pain medications. Many other modalities for hurting control like TENS, acupuncture, stretching, exercise, and yoga can help.
Outcomes
Overall the outcomes after surgery are not satisfactory; the surgery is often associated with astringent complications that are worse than scoliosis itself. In addition, many patients accept depression self-esteem because of the spinal defect and remain isolated and withdrawn. The interprofessional team should take steps to ensure that they do not offer invasive treatments that are more than probable to exercise more than impairment than good; the key is to improve the quality of life.[12][xiii][14] (Level Five)
(Click Image to Overstate)
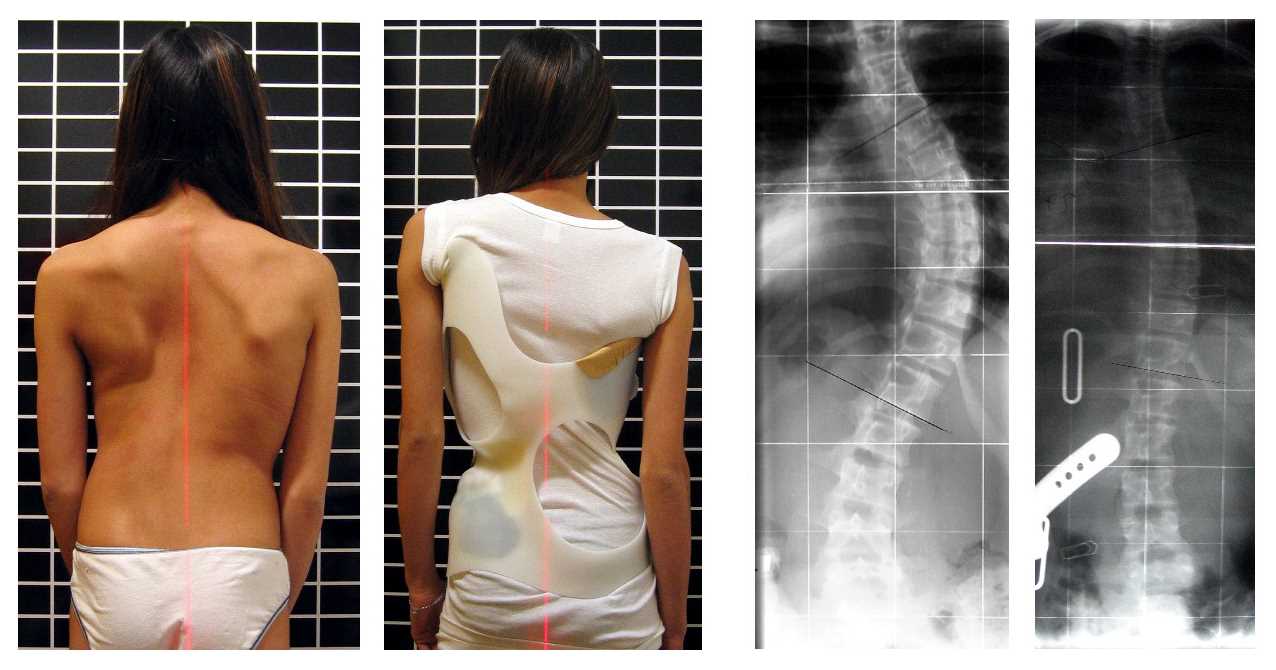
Scoliosis patient in Chêneau brace correcting from 56° to 27° Cobb (chief correction of 52%).
Contributed by Wikimedia Commons, Weiss HR (CC past ii.0) https://creativecommons.org/licenses/by/ii.0/
(Click Epitome to Enlarge)
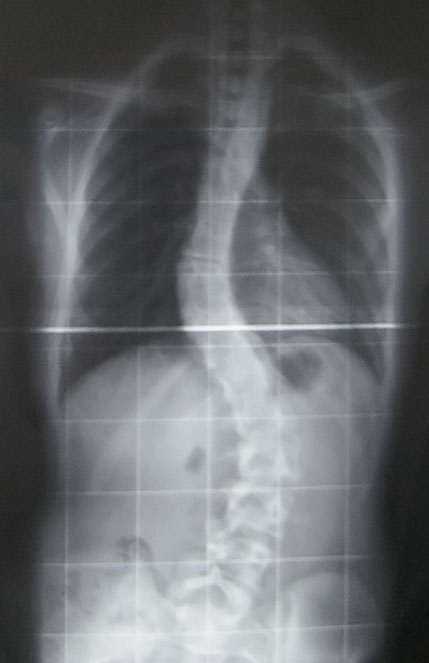
This is an posterior-to-anterior X-ray of a case of boyish idiopathic scoliosis - specifically, my spine. There is a thoracic curve of 30° and a lumbar bend of 53° (Cobb angle - meet scoliosis). This was taken at the Royal National Orthopaedic Hospital. The largest curve (53°) is of a magnitude typically near the lower surgery boundary, although many factors decide whether surgery is necessary on a scoliosis case.
Contributed past Wikimedia Eatables (Public Domain)
(Click Image to Enlarge)

scoliosis of the spine
Image courtesy S Bhimji MD
(Click Image to Overstate)

Scoliosis of the spine
Contributed by Sunil Munakomi, MD
References
[i]
Fruergaard S,Ohrt-Nissen S,Dahl B,Kaltoft Due north,Gehrchen M, Neural Axis Abnormalities in Patients With Adolescent Idiopathic Scoliosis: Is Routine Magnetic Resonance Imaging Indicated Irrespective of Curve Severity? Neurospine. 2019 Jun [PubMed PMID: 30653908]
[2]
Pepke W,Almansour H,Lafage R,Diebo BG,Wiedenhöfer B,Schwab F,Lafage V,Akbar M, Cervical spine alignment post-obit surgery for adolescent idiopathic scoliosis (AIS): a pre-to-post analysis of 81 patients. BMC surgery. 2019 Jan 15 [PubMed PMID: 30646880]
[iii]
Zhu H,Li B,Jian Y,Dominicus Z,Yang Z, [Effectiveness analysis of Lenke type 1 adolescent idiopathic scoliosis with different proximal fixation vertebra]. Zhongguo xiu fu chong jian wai ke za zhi = Zhongguo xiufu chongjian waike zazhi = Chinese journal of reparative and reconstructive surgery. 2019 Jan 15 [PubMed PMID: 30644259]
[4]
Yagci K,Yakut Y, Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment. Prosthetics and orthotics international. 2019 Jan ten; [PubMed PMID: 30628526]
[5]
Levi D,Springer Due south,Parmet Y,Ovadia D,Ben-Sira D, Acute muscle stretching and the ability to maintain posture in females with adolescent idiopathic scoliosis. Journal of back and musculoskeletal rehabilitation. 2019 Jan 4; [PubMed PMID: 30636726]
[half-dozen]
van den Bogaart M,van Royen BJ,Haanstra TM,de Kleuver M,Faraj SSA, Predictive factors for brace handling outcome in adolescent idiopathic scoliosis: a best-evidence synthesis. European spine journal : official publication of the European Spine Club, the European Spinal Deformity Gild, and the European Department of the Cervical Spine Enquiry Society. 2019 Jan 3; [PubMed PMID: 30607519]
[8]
Grabala P,Helenius I,Buchowski JM,Larson AN,Shah SA, Back Pain and Outcomes of Pregnancy After Instrumented Spinal Fusion for Boyish Idiopathic Scoliosis. World neurosurgery. 2019 Jan three [PubMed PMID: 30610987]
[nine]
Le Berre Thousand,Pradeau C,Brouillard A,Coget 1000,Massot C,Catanzariti JF, Do Adolescents With Idiopathic Scoliosis Accept an Erroneous Perception of the Gravitational Vertical? Spine deformity. 2019 Jan [PubMed PMID: 30587324]
[10]
Farooqui SI,Siddiqui PQR,Ansari B,Farhad A, Furnishings of spinal mobilization techniques in the management of boyish idiopathic scoliosis - A meta-analysis. International periodical of health sciences. 2018 Nov-December; [PubMed PMID: 30534043]
[11]
Lonstein JE, Selective Thoracic Fusion for Boyish Idiopathic Scoliosis: Long-Term Radiographic and Functional Outcomes. Spine deformity. 2018 Nov - Dec; [PubMed PMID: 30348342]
[12]
Chang DG,Suk SI,Kim JH,Vocal KS,Suh SW,Kim SY,Kim GU,Yang JH,Lee JH, Long-term Consequence of Selective Thoracic Fusion Using Rod Derotation and Directly Vertebral Rotation in the Treatment of Thoracic Adolescent Idiopathic Scoliosis: More Than x-Year Follow-up Data. Clinical spine surgery. 2019 Jun eighteen; [PubMed PMID: 31220038]
[xiii]
Diebo BG,Segreto FA,Solow M,Messina JC,Paltoo Thousand,Burekhovich SA,Flower LR,Cautela FS,Shah NV,Passias PG,Schwab FJ,Pasha S,Lafage 5,Paulino CB, Adolescent Idiopathic Scoliosis Care in an Underserved Inner-Metropolis Population: Screening, Bracing, and Patient- and Parent-Reported Outcomes. Spine deformity. 2019 Jul; [PubMed PMID: 31202371]
[14]
Weinstein SL, The Natural History of Adolescent Idiopathic Scoliosis. Journal of pediatric orthopedics. 2019 Jul; [PubMed PMID: 31169647]
Source: https://www.statpearls.com/ArticleLibrary/viewarticle/686
0 Response to "The Nurse Reviews the Pathophysiology of Scoliosis With the Student Nurses"
Post a Comment